Ethical Challenges and Considerations in One Health Approaches to Emerging Infectious Diseases: A Descriptive Review
1Faculty of Public Health, Department of Environmental Health, Universitas Indonesia, Depok, Indonesia
2School of Bioengineering, Dalian University of Technology, China
3Faculty of Public Health, Department of Occupational Health and Safety, Universitas Indonesia (UI), Depok, Indonesia
4Department of Microbiology, Faculty of Medicine, Universitas Indonesia (UI), Jakarta, Indonesia
© 2026 Bio Communications
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Abstract
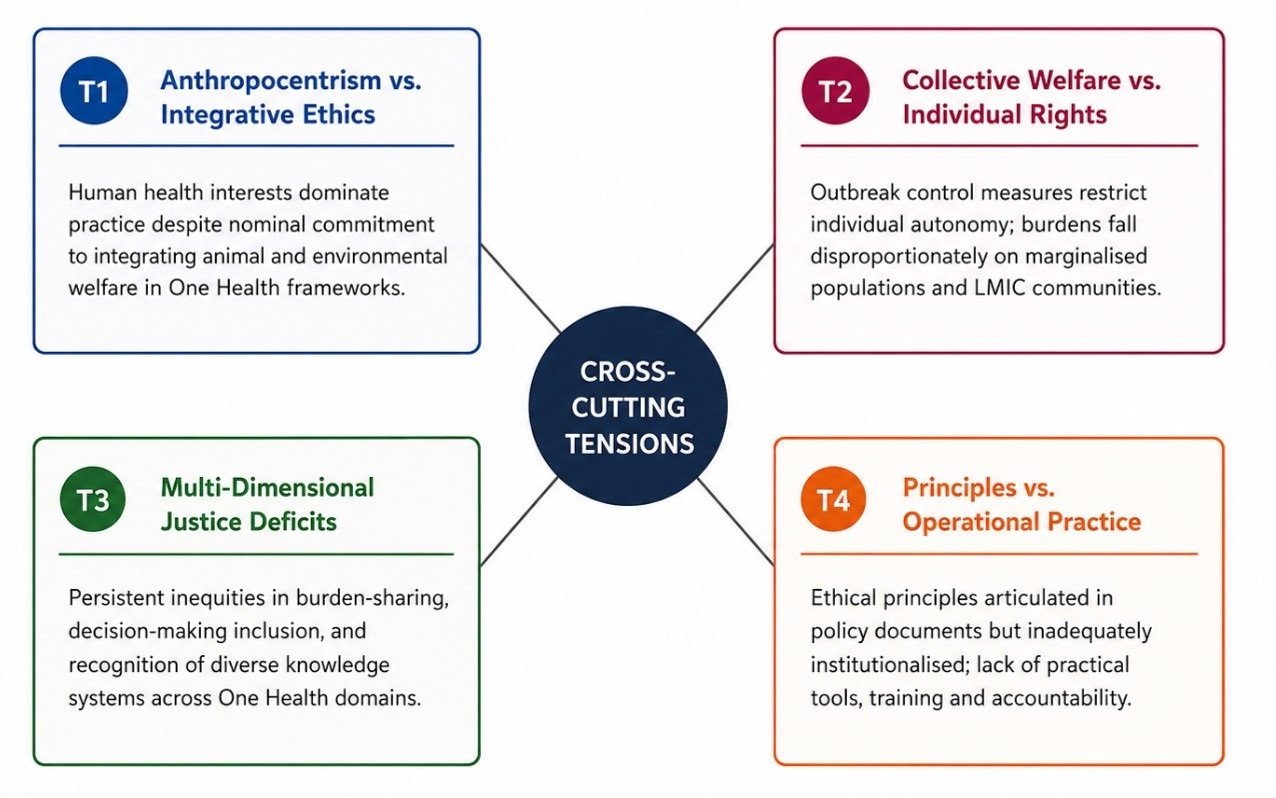
The One Health framework has emerged as a central paradigm for addressing emerging infectious diseases (EIDs) by recognizing the interconnectedness of human, animal, and environmental health. Despite increasing global adoption, the ethical dimensions of One Health remain conceptually fragmented and inconsistently operationalized across research, governance, and policy. This descriptive review synthesizes ethical challenges associated with One Health approaches to EIDs across six interrelated domains: animal ethics and welfare, public health ethics, environmental and planetary ethics, governance and policy, research ethics in outbreak settings, and emerging ethical frameworks. Drawing on peer-reviewed literature, policy documents, and conceptual scholarship, the review identifies four major cross-cutting ethical tensions. First, anthropocentric priorities continue to dominate One Health implementation, subordinating animal welfare and ecological integrity to human-centered outcomes. Second, tensions between collective welfare and individual rights become acute during outbreaks, imposing disproportionate burdens on marginalized populations. Third, persistent distributive, procedural, and epistemic injustices shape global and local responses, especially affecting low- and middle-income countries, indigenous communities, and non-human populations. Fourth, a substantial implementation gap exists between the articulation of ethical principles and their translation into enforceable institutional practice. The review further incorporates emerging ethical challenges related to antimicrobial resistance (AMR) within One Health contexts, empirical evidence from major outbreaks including COVID-19, Ebola, and avian influenza, and perspectives from Global South scholarship to address equity dimensions. Emerging frameworks, including One Health Ethics, Planetary Health Ethics, ethics of care, indigenous relational ethics, and epistemic justice approaches, offer promising foundations for more inclusive governance, yet remain insufficiently integrated into operational decision-making. The review argues that One Health ethics must evolve into a rigorous interdisciplinary field supported by practical governance tools, equitable research frameworks, transparent accountability mechanisms, and inclusive policymaking. Without such developments, the transformative potential of One Health will remain ethically and institutionally constrained.
Keywords:
One Health, emerging infectious diseases, animal welfare, public health ethics, environmental ethics, governance
1. Introduction
The emergence and re-emergence of infectious diseases at the human–animal–environment interface represents one of the defining public health challenges of the twenty-first century. Diseases such as Severe Acute Respiratory Syndrome (SARS), Middle East Respiratory Syndrome (MERS), Ebola virus disease, avian influenza, Nipah virus infection, and most recently COVID-19 have demonstrated with force that pathogens do not respect disciplinary or jurisdictional boundaries (Morse et al., 2012). Approximately 60% of known human infectious diseases are zoonotic in origin, and an estimated 75% of emerging infectious diseases arise from animal reservoirs (Jones et al., 2008). These epidemiological realities have catalysed growing scientific and policy interest in the One Health framework, an integrative approach that recognizes the inextricable connections among human health, animal health, and ecosystem integrity.
The One Health concept has been formally endorsed by major international organizations including the World Health Organization (WHO), the Food and Agriculture Organization of the United Nations (FAO), the World Organization for Animal Health (WOAH, formerly OIE), and the United Nations Environment Program (UNEP), which together constitute the Quadripartite alliance for One Health implementation (One Health High-Level Expert Panel [OHHLEP], 2022). While the scientific and operational dimensions of One Health have attracted considerable scholarly attention, the ethical dimensions of implementing this framework in the context of emerging infectious diseases (EIDs) remain comparatively underdeveloped. This gap is significant because ethical questions permeate every aspect of One Health practice, from surveillance design and research methodology to resource allocation, animal management, environmental governance, and community engagement (Degeling et al., 2015).
Ethics in One Health is not a peripheral concern; it is foundational. Decisions about how to balance human health protection against animal welfare interests, how to govern environmental interventions with ecological consequences, how to conduct ethically sound research during rapidly evolving outbreaks, and how to ensure equitable treatment of diverse human and non-human stakeholders all reflect deeply contested moral values. Yet, despite the breadth of these challenges, no comprehensive descriptive synthesis of the ethical landscape across the full scope of One Health practice as it pertains to EIDs, currently exists. Existing reviews tend to address discrete ethical issues in isolation, without situating individual concerns within the broader One Health ethical architecture.
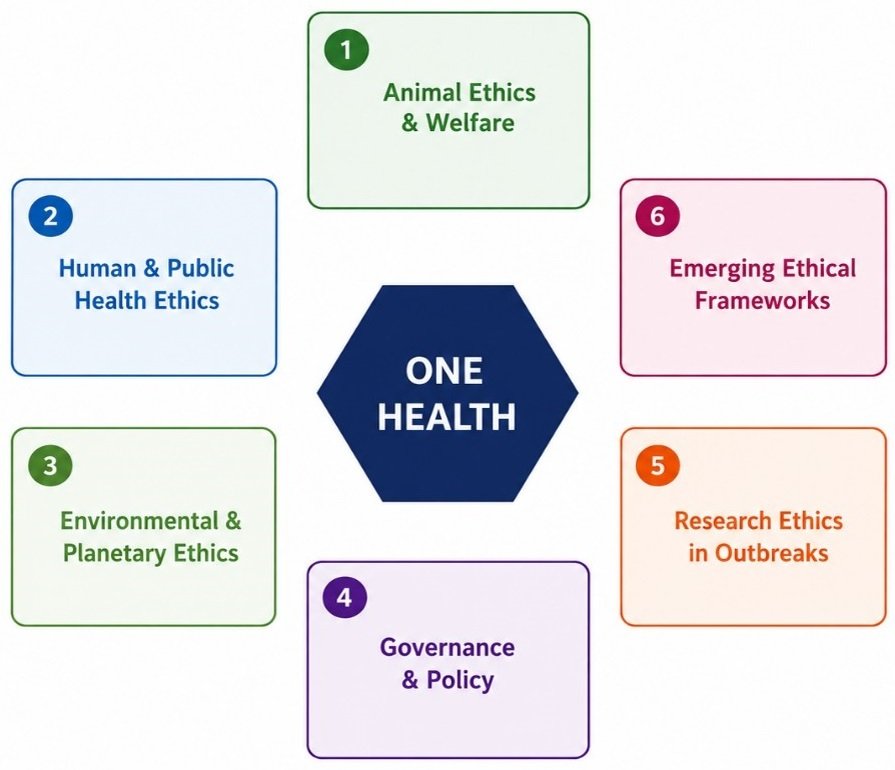
The present article addresses this gap by providing a structured descriptive review of ethical challenges and considerations across six interrelated domains of One Health approaches to EIDs. Additionally, ethical dimensions of antimicrobial resistance (AMR) within One Health frameworks are integrated throughout this review, as AMR represents a critical inter-sectoral challenge linking human medicine, veterinary practice, and environmental stewardship. AMR exemplifies the quintessential One Health ethical dilemma: individual therapeutic benefit versus collective ecological harm, with disproportionate consequences for LMICs that lack robust regulatory infrastructure (Msemakweli et al., 2024). Drawing on peer-reviewed literature, policy documents, and conceptual analyses, this review maps the ethical terrain of One Health practice, identifies recurring tensions and knowledge gaps, and highlights the need for more robust, inclusive, and practically applicable ethical frameworks (Fig. 1).
The paper is structured as follows. Section 2 presents methods, including literature search strategy and scope and inclusion/exclusion criteria. Section 3 examines animal ethics and welfare. Section 4 addresses human and public health ethics. Section 5 explores environmental and planetary ethics. Section 6 analyzes governance and policy dimensions. Section 7 reviews research ethics in outbreak settings. Section 8 discusses emerging ethical frameworks. A synthesising discussion and conclusion are presented in Sections 9 and 10, respectively.
2. Methodology
This study was conducted as a descriptive narrative review aimed at synthesizing ethical challenges and considerations associated with One Health approaches to emerging infectious diseases (EIDs). Literature was identified through structured searches of PubMed, Scopus, Web of Science, and Google Scholar between January and March 2025. Search terms included combinations of: “One Health, ethics, bioethics, animal welfare, public health ethics, environmental ethics, planetary health, governance, research ethics, emerging infectious diseases, zoonoses, outbreaks, and pandemics".
Peer-reviewed articles, policy reports, institutional documents, and conceptual papers published in English were considered eligible if they addressed ethical dimensions of One Health, zoonotic diseases, outbreak response, governance, animal welfare, environmental health, or related ethical frameworks. Studies focused solely on biomedical or epidemiological outcomes without substantive ethical discussion were excluded. Literature selection was conducted through title, abstract, and full-text screening. Given the conceptual nature of the review, emphasis was placed on relevance, influence within the field, and contribution to ethical discourse rather than quantitative quality assessment. Relevant grey literature from international organizations, including WHO, FAO, WOAH, UNEP, and OHHLEP, was also reviewed to capture contemporary policy developments. The identified literature was synthesized thematically and organized into six major ethical domains: animal ethics and welfare, public health ethics, environmental and planetary ethics, governance and policy, research ethics in outbreak settings, and emerging ethical frameworks.
3. Animal Ethics and Welfare
Animal ethics and welfare represent central concerns that cut across biomedical research, zoonotic disease control, disaster management, companion animal policy, livestock technology, and environmental thinking (Blaxter et al., 2024). Collectively, the literature reveals a clear shift away from narrow anthropocentric models, in which animals are valued primarily for their instrumental utility to humans, toward broader frameworks that recognize animals as beings with intrinsic value, welfare interests, and ecological significance (ten Have & Patrão Neves, 2021). At the same time, the evidence reveals unresolved ethical tensions between care and control, scientific progress and moral responsibility, individual welfare and ecosystem protection, and technological innovation and justice (Criscuolo & Sueur, 2020).
A foundational concern is that the ethical treatment of animals cannot be separated from the quality and purpose of the systems in which they are used. In the context of biomedical animal research, the literature argues that animal suffering cannot be ethically justified simply because research claims to benefit society (Díaz et al., 2021). Scientific quality thereby becomes an ethical issue in itself: if research is weak, poorly designed, or unlikely to produce meaningful benefit, the harms imposed on animal subjects lose moral legitimacy. The proposed Harm Yield Analysis strengthens this argument by suggesting that ethical review should assess not only harm to animals and potential social benefit, but also the methodological rigor and validity of the research design. This reveals a significant gap in many existing frameworks, which evaluate ethical concerns without adequately integrating scientific quality assessment (Brill et al., 2019).
The literature further expands animal ethics beyond research settings by examining how public attitudes and moral emotions shape the management of animals in society. Debates over community cat management and trap-neuter-return (TNR) programs illustrate a broader shift from lethal control toward more compassionate approaches grounded in zoocentric and virtue-based ethics (Wolf & Schaffner, 2019). Care, empathy, and recognition of animals’ intrinsic value are central to these approaches; however, ongoing debates about balancing individual animal welfare with wildlife protection, disease control, and community interests highlight that such conflicts involve competing moral responsibilities rather than straightforward right or wrong answers (De Briyne et al., 2020).
This tension becomes considerably more complex in the context of zoonotic diseases and One Health. Animals appear simultaneously as vulnerable beings with welfare interests and as components of disease networks linking humans, animals, and environments. The literature firmly rejects the framing of zoonoses as purely veterinary or biomedical problems, describing them instead as systemic issues shaped by climate change, environmental degradation, human behavior, social inequality, and economic structures (Mertz et al., 2024). This broadening of the frame significantly expands the ethical discussion: disease prevention concerns not only human safety but also fairness between humans and animals, and the ethical implications of practices such as mass culling, intensive confinement, and heavy antimicrobial use across industrial livestock systems.
The ethics of care perspective, applied to animal disaster management, adds a relational dimension to welfare analysis (Anthony & De Paula Vieira, 2022). Rather than treating animals as secondary considerations during crises, this approach emphasizes shared vulnerability, interdependence, and interspecies solidarity. It contends that the experiences of animals during disasters carry genuine moral weight and should inform preparedness, response, and recovery planning. Within the broader One Health framework, animal behavior and welfare research similarly argues that animal wellbeing deserves consideration equal to human and environmental health and highlights the need to include marginalized perspectives and to better represent animals’ welfare through their behavior and lived experience (Yeates, 2024).
3.1 Antimicrobial Resistance and Animal Ethics
The ethics of antimicrobial use in livestock production represents one of the most pressing and under-addressed dimensions of animal ethics within One Health. The routine use of antimicrobials in industrial animal farming for growth promotion and prophylaxis contributes substantially to the global burden of AMR, generating externalities that fall disproportionately on human communities in LMICs and on future generations. Ethically, this practice exemplifies a conflict between short-term commercial interest and long-term collective welfare, raising questions of intergenerational justice, corporate responsibility, and regulatory failure (Van Boeckel et al., 2014). Several LMIC governments, including India and South Africa, have introduced regulatory frameworks to limit agricultural antimicrobial use, but enforcement capacity and industry resistance remain significant barriers. The One Health framework is uniquely positioned to address AMR through coordinated intersectoral governance, yet most existing AMR action plans remain siloed within either human health or veterinary regulatory domains, rather than integrated across both(Organization). Advancing AMR ethics within One Health requires explicit attention to the political economy of food production, the rights of communities affected by AMR, and the equitable distribution of the cost of transition to more sustainable agricultural practices.
The emergence of artificial intelligence (AI) applications in livestock farming introduces a newer but rapidly expanding ethical frontier. While digital technologies are frequently promoted as tools for enhancing efficiency and welfare monitoring, ethical reflection has lagged significantly behind implementation. The absence of developed ethical frameworks and codes of conduct for AI in livestock contexts represents a critical gap.
Finally, critique of anthropocentric models of animal ethics challenges the field at a more fundamental level. Even apparently progressive ethical frameworks frequently privilege animals according to human-like traits such as sentience, cognitive complexity, or emotional familiarity, thereby reproducing hierarchies of moral consideration that marginalize ecologically important but less cognitively conspicuous species (Rodriguez, 2024).
4. Human and Public Health Ethics
Human and public health ethics occupies a central position within One Health approaches to EIDs, as the protection of human populations has historically been the primary driver of surveillance, policy, and response. However, the ethical principles underpinning public health practice, namely beneficence, non-maleficence, justice, autonomy, and solidarity, are not always easily reconciled in outbreak contexts, and their application within a One Health framework introduces additional complexity relating to competing interests across human, animal, and environmental health (Dawson & Jennings, 2012).
One of the most persistent ethical tensions in public health responses to EIDs concerns the balance between individual rights and collective welfare. Outbreak control frequently requires measures that constrain individual autonomy, including quarantine, isolation, mandatory treatment, travel restrictions, and surveillance, to protect the broader population. The ethical justification for such restrictions rests on a utilitarian calculation that weighs collective benefit against individual liberty, but this calculation is rarely straightforward (Selgelid, 2009). During the SARS outbreak of 2002-2003, quarantine measures imposed significant psychological, social, and economic burdens on affected individuals and communities, raising questions about the proportionality of public health interventions and the adequacy of support for those whose freedoms were curtailed (Hawryluck et al., 2004). Similar tensions recurred during the COVID-19 pandemic, wherein sweeping public health restrictions disproportionately burdened marginalized and economically vulnerable populations, exposing deep structural inequities in the distribution of pandemic costs and benefits (Bambra et al., 2020).
Justice constitutes a second major axis of ethical concern in One Health public health practice. Emerging infectious diseases do not affect all human populations equally; rather, they cluster in settings characterized by poverty, inadequate sanitation, high-density livestock keeping, limited healthcare access, and ecological disruption (Patz et al., 2004). The principle of distributive justice demands that public health responses address not only immediate disease burdens but also the underlying social determinants that render certain populations disproportionately vulnerable. Within a One Health framework, this extends to recognising that communities in close proximity to wildlife or in agricultural settings, particularly in low- and middle-income countries (LMICs), bear the greatest risk from EIDs while typically having the least access to protective resources (Grace et al., 2012). Failure to address these inequities perpetuates existing patterns of global health injustice.
The principle of solidarity enriches the ethical analysis of One Health public health responses by foregrounding mutual obligation and collective responsibility in the face of shared vulnerability (Prainsack & Buyx, 2012). International cooperation in EID control depends on the willingness of countries to share pathogen samples, surveillance data, and medical countermeasures. However, this cooperation has been undermined repeatedly by disputes over equitable access, most notably the controversies over H5N1 influenza sample sharing under the Pandemic Influenza Preparedness Framework and, subsequently, the pronounced inequities in COVID-19 vaccine distribution. These episodes reveal that solidarity in global health is contested and unevenly practised, and that One Health governance must grapple seriously with the ethical obligations of high-income countries toward LMICs in the context of shared infectious disease threats.
Stigmatisation represents a further ethical challenge in One Health EID responses. Public health communication during outbreaks has at times reinforced harmful associations between specific ethnic, occupational, or geographic communities and disease risk, contributing to discrimination, social exclusion, and reduced engagement with health services (Bavel et al., 2020). The labeling of COVID-19 as a “Chinese virus,” the stigmatisation of bushmeat traders and bat hunters during Ebola outbreaks, and the historical association of specific social groups with HIV/AIDS illustrate how disease narratives can be weaponised in ways that simultaneously undermine ethical obligations of non-discrimination and the practical goals of outbreak containment, since stigmatisation deters affected individuals from disclosing symptoms or seeking care.
Communication ethics, encompassing transparency, honesty, and the responsible management of scientific uncertainty, constitutes a final critical dimension. Public health authorities face difficult decisions about when and how to communicate risk, particularly when evidence is incomplete or evolving rapidly (Fischhoff, 2012). Excessive caution can generate panic and erode institutional trust, while premature reassurance may produce under-preparedness. Ethical communication requires honest acknowledgment of uncertainty, provision of actionable guidance based on available evidence, and the engagement of communities as active participants in, rather than passive recipients of, public health messaging. In One Health contexts, this challenge is amplified by the need to communicate across multiple professional sectors and to audiences with varying health literacy and culturally diverse frameworks for understanding disease causation and risk.
5. Environmental and Planetary Ethics
The One Health concept seeks to achieve an integrated approach to human, animal, and environmental health. However, the ethics of environment and planetary justice within One Health are not yet fully elaborated. While the framework may contribute to bridging anthropocentrism by recognising the interdependence between species through the acknowledgment of environmental linkages, recent analyses show that in practice, anthropocentric perspectives are preserved through the consistent prioritization of human health outcomes (Sheather, 2023).
Although this review identifies anthropocentrism as a persistent limitation of One Health implementation, prioritizing human health during acute public health emergencies may sometimes be ethically justified. During severe outbreaks such as Ebola, H1N1 influenza, and COVID-19, the immediate protection of human life may require difficult trade-offs involving animal welfare and environmental considerations. The ethical challenge is therefore not the temporary prioritization of human health during emergencies, but the continued dominance of anthropocentric approaches in routine governance and long-term policy (Diller & Williamson, 2023; Van Herten, 2021). A mature One Health ethics should balance the legitimate demands of emergency response with sustained commitments to animal welfare, ecological integrity, and interspecies justice.
Climate change and disease management illustrate the need to address ethico-political issues associated with environmental manipulation, such as the deployment of Wolbachia-infected mosquitoes for the control of climate-susceptible vector-borne diseases. Such innovations entail unresolved ethical questions concerning ecosystem manipulation, the precautionary principle in relation to non-human species, and the moral status of affected organisms (Sheather, 2023).
A significant structural limitation concerns the balance of One Health data systems. Human and human-animal surveillance data currently form the primary basis for modern monitoring systems, while the number of environmental and plant-related biomonitoring indicators remains comparatively low. This imbalance affects risk assessment and the setting of national and international policies (Basheer et al., 2025). Ethical dilemmas arising from interventions used to control zoonotic diseases have similarly attracted insufficient attention in the One Health literature. Analysis of current practices and their ethical implications suggests that public health interests are systematically afforded precedence over animal welfare and environmental concerns, a pattern rooted in deeply embedded anthropocentric governance styles. Although emergency measures may be justified under conditions of genuine uncertainty, the absence of explicit ethical principles for navigating trade-offs between competing values diminishes the transparency and moral legitimacy of One Health practice (van Herten et al., 2020).
The relationship between biodiversity loss and emerging infectious disease carries distinct ethical weight that remains underexplored in One Health discourse. Empirical evidence increasingly links habitat fragmentation, species loss, and land-use intensification with increased spillover risk from wildlife reservoirs to human populations (Jones et al., 2008). The ethical implication is profound: the exploitation of natural environments for agricultural expansion, extractive industry, and urban development not only degrades ecosystems but actively generates the conditions for pandemic emergence. This positions EID risk as partly a consequence of choices made by actors in high-income countries whose consumption patterns drive deforestation and biodiversity loss in LMICs, a dynamic that raises questions of causal responsibility, distributive justice, and the obligation of wealthier nations to support ecological restoration in regions most affected by land-use-driven disease emergence.
Intergenerational equity constitutes a further moral dimension that environmental ethics within One Health has yet to systematically address. Current environmental governance decisions (relating to deforestation rates, wetland drainage, freshwater contamination, and climate emissions) impose health risks on future generations who bear no responsibility for the choices that created them. A genuinely planetary ethics, as articulated within the Rockefeller Foundation-Lancet Commission on planetary health, holds that decision-makers are morally obliged to account for long-term ecological and epidemiological consequences, not merely immediate public health gains (Whitmee et al., 2015). This demands systematic integration of future-oriented ethical analysis into environmental governance under the One Health framework, including precautionary approaches to ecological interventions whose long-term consequences cannot be adequately modelled with existing tools.
Climate justice adds a further layer of ethical complexity to environmental governance in One Health. Climate change alters the geographic range and seasonal patterns of vector-borne diseases, intensifies drought and flooding events that compromise sanitation and water quality, and disrupts agricultural systems in ways that increase human-wildlife contact. LMICs, which have contributed least to cumulative greenhouse gas emissions, bear disproportionate climate-related disease burdens. This asymmetry creates a moral obligation for high-income countries, under the principles of common but differentiated responsibilities, to invest substantially in the climate adaptation capacities of health systems in vulnerable regions. One Health governance frameworks that fail to engage with climate justice thereby reproduce the same structural inequities they are ostensibly designed to address.
The legal recognition of the rights of nature, while still at early stages of institutional development, opens a significant avenue for operationalising environmental ethics within One Health. Constitutional provisions recognising ecosystem rights in Ecuador and Colombia, judicial recognition of the rights of rivers in India and New Zealand, and emerging legal scholarship on non-human legal standing collectively suggest that rights-based approaches may provide enforceable mechanisms for constraining environmentally harmful practices that increase EID risk (Knox, 2017). Incorporating rights-of-nature frameworks into One Health governance would represent a substantial shift from the current instrumentalisation of environmental considerations toward a genuinely non-anthropocentric ethical architecture.
In summary, environmental ethics within One Health appears to be powerfully endorsed in declaratory statements but inadequately implemented in operational practice. To resolve this inconsistency, governance frameworks must articulate in concrete and enforceable terms how ecological integrity, animal welfare, and intergenerational equity are to be incorporated into routine operational decision-making. Without such specificity, environmental ethics risks remaining aspirational rather than transformative.
6. Governance and Policy
From an institutional and ethical perspective, One Health presents both significant opportunities and complex governance challenges. Among the most pressing is global health equity. In low- and middle-income countries, health infrastructure, human resource capacity, and budgetary resources are frequently inadequate for the implementation of effective One Health-based surveillance and response systems, thereby exacerbating existing inequities. The equitable distribution of One Health-related funding, the strengthening of health system capacities, and more coordinated access to financial resources are necessary conditions for avoiding the perpetuation of structural asymmetries and the creation of new forms of dependency that undermine national ownership and local sovereignty (Zhou et al., 2024).
6.1 LMIC Governance Perspectives
Global One Health governance frameworks have been disproportionately shaped by the epistemic and institutional priorities of high-income countries, a pattern that reflects and reproduces colonial asymmetries in global health governance (Lainé, 2023). African, Asian, and Latin American scholars have increasingly challenged the assumption that One Health frameworks developed in European and North American institutional contexts are universally applicable, arguing that locally embedded approaches attentive to context-specific human-animal relationships, livelihood structures, and epistemic traditions are both more ethical and more effective (Estebanez & Boireau, 2022; Lee & Brumme, 2013). For example, in East African pastoral communities, human-livestock-wildlife interfaces are governed by indigenous ethical systems that encode sophisticated understandings of interspecies reciprocity and ecological stewardship—systems that are rarely acknowledged in formal One Health governance frameworks despite their demonstrated effectiveness in managing zoonotic risk over centuries. Ethical governance of One Health in these contexts requires not merely the inclusion of LMIC voices in existing institutional structures but the genuine reconstitution of governance frameworks to center local knowledge, authority, and accountability (Estebanez & Boireau, 2022).
6.2 Practical Governance Tools and Operationalization
Recognizing the persistent gap between ethical principle and institutional practice, several practical tools have been developed or proposed to operationalize One Health ethics in governance contexts. First, the One Health Joint Plan of Action, developed by the Quadripartite, provides a governance architecture for intersectoral coordination, though it currently lacks explicit ethical performance indicators. Second, the Joint External Evaluation (JEE) tool, used by WHO to assess national health security capacities under the International Health Regulations (Machalaba et al., 2018), could be expanded to incorporate One Health ethics metrics, including indicators of community participation, indigenous knowledge integration, and animal welfare governance. Third, the development of One Health ethics review committees modeled on institutional review boards but constituted to include veterinarians, ecologists, ethicists, community representatives, and indigenous knowledge holders has been proposed as a mechanism for embedding ethical deliberation in routine One Health governance (Rüegg et al., 2017). Fourth, participatory impact assessment frameworks that explicitly evaluate the distributional consequences of One Health interventions across human, animal, and environmental beneficiaries would provide governance bodies with tools for identifying and addressing ethical trade-offs before implementation rather than retrospectively. The adoption of any such tools, however, requires both political will and sustained funding resources that must be committed by high-income countries and international institutions as a matter of global health justice.
The International Health Regulations (IHR, 2005) constitute the primary international legal instrument for governing state responses to public health emergencies of international concern. However, their application within a One Health context reveals significant ethical limitations. The IHR framework is structured around human health endpoints and state-centric notification obligations, providing minimal guidance on how animal health events and environmental signals should be integrated into official surveillance and reporting chains.
Accountability and evaluation mechanisms in One Health governance remain underdeveloped. Most existing frameworks specify process goals, including the formation of multi-sectoral committees, the adoption of joint work plans, and the conduct of intersectoral exercises, without providing enforceable standards for ethical outcomes such as the equitable distribution of resources, the meaningful participation of marginalized communities, or the demonstrable integration of animal and environmental welfare into decision-making. Developing ethically grounded performance metrics for One Health governance, including indicators of procedural fairness, epistemic inclusion, and ecological accountability, represents a critical priority for future policy development.
7. Research Ethics in Outbreaks
Research ethics in outbreak settings poses challenges that are not entirely unique to One Health but that acquire distinctive features in intersectoral, multispecies contexts. To clarify the One Health-specific dimensions: standard outbreak research ethics addresses issues of expedited consent, vulnerable populations, and data sharing in human health contexts. One Health research ethics uniquely confronts additional challenges including (1) the simultaneous governance of research across human, animal, and environmental domains under jurisdictions with distinct ethical standards; (2) the inclusion of community animal owners and pastoralists as research participants with complex interests in both human and animal health outcomes; (3) the ethical implications of wildlife sampling and environmental monitoring without the capacity for meaningful consent; and (4) the governance of data generated about non-human subjects in contexts where standard research ethics frameworks provide no guidance. These distinctive features require that One Health ethics develop specific supplementary standards rather than simply applying existing human research ethics frameworks to inter-sectoral contexts.
Disease outbreaks constitute acute public health crises in which timely research is essential for understanding disease dynamics and identifying effective interventions. Research conducted during outbreaks generates critical evidence on transmission patterns, clinical management, and prevention strategies (Damon, 2018). Nevertheless, the conduct of research in outbreak settings generates distinct and significant ethical challenges. The imperative to produce timely evidence must be carefully balanced against the responsibility to protect research participants and to maintain the fairness and integrity of scientific inquiry (Han et al., 2020). Ethics therefore assumes a central role in guiding the design and implementation of research conducted under conditions of health emergency (Haskins, 2020).
Maintaining adequate research oversight during rapidly evolving outbreaks is among the most substantial ethical challenges. Conventional research approval procedures may involve extended timelines that risk delaying the initiation of critical studies (Aarons, 2019). Ethical review bodies must therefore develop mechanisms for thorough yet expedited review that do not compromise participant protections. Scholars have highlighted the value of pre-developed adaptable research protocols and streamlined ethical review processes that can be activated at the onset of outbreaks (Saxena et al., 2019). Such preparedness mechanisms enable researchers to act with the requisite speed while ensuring that research is conducted in accordance with established ethical standards.
Informed consent represents another fundamental ethical dimension of outbreak research. Individuals affected by outbreaks frequently experience heightened fear, informational uncertainty, and limited access to credible guidance, all of which can compromise autonomous decision-making (Nichol & Antierens, 2021). Researchers are obliged to explain the purpose, risks, and anticipated benefits of studies clearly and transparently (Mormina et al., 2024). The assurance of genuinely voluntary participation is particularly critical in emergency settings, where perceived coercive pressures may arise from limited treatment alternatives. Ethical research practice requires that participants be explicitly informed that their participation is not obligatory and that they retain the right to withdraw at any time without consequence (Bianchi, 2022; Nouvet et al., 2022). Linguistic and cultural adaptation of consent procedures is essential to ensuring that participants can exercise meaningful informed choice.
The use of experimental interventions raises further ethical concerns in outbreak settings. When diseases emerge for which no approved treatments or vaccines are available, investigational products may be considered for deployment through clinical trials or emergency use authorisations (Asundi & Bhadelia, 2020; Edwards & Kochhar, 2020). While such interventions may offer hope in critical situations, their safety and efficacy profiles remain uncertain by definition. Ethical principles require that only interventions with a reasonable scientific foundation be applied, that risks be critically assessed, and that participants be fully informed of the experimental nature of the intervention and associated uncertainties (Lane et al., 2016). Concurrently, research designs must be sufficiently rigorous to generate credible, generalisable evidence for future public health responses.
Equity constitutes an additional ethical imperative in outbreak research. The majority of infectious disease outbreaks occur in low-resource settings with limited healthcare infrastructure and research capacity. Ethical principles demand that affected communities be genuine participants in research rather than merely sites of data collection (Ravinetto et al., 2024). Collaboration with local researchers and public health authorities helps ensure that studies are responsive to local needs and culturally appropriate (Folayan et al., 2019). Meaningful community engagement builds trust, enhances participation, and improves the relevance of research activities. Moreover, ethical standards require that communities who contribute to research derive tangible benefits from its outcomes, including improved healthcare access or strengthened health system capacity.
Transparent and responsible data sharing represents a final critical ethical concern during outbreaks (Kallas & O’Connor, 2016). The rapid sharing of research findings can substantially advance global response efforts by informing public health strategies and accelerating the development of diagnostics, treatments, and vaccines (Littler, 2017). Ethical guidelines encourage timely sharing of epidemiological and clinical information between researchers and health authorities. However, data sharing must be balanced against the protection of participant privacy and the responsible stewardship of sensitive health information. Clear governance structures for data use and sample storage are essential to maintaining the trust of participants and communities.
8. Emerging Ethical Frameworks
The ethical challenges catalogued across the preceding sections collectively underscore the limitations of existing frameworks when applied to the complex, multi-species, multi-sectoral realities of One Health approaches to EIDs. In response, a number of emerging frameworks have been proposed that seek to move beyond conventional bioethical principles toward more integrative, relational, and justice-oriented approaches (Degeling et al., 2015; Rodriguez, 2024).
Among the most influential is One Health Ethics, conceived as a distinct sub-discipline that extends traditional medical and public health ethics to encompass the moral relationships between humans, animals, and ecosystems. Proponents argue that existing frameworks, rooted in principles of autonomy, beneficence, non-maleficence, and justice as applied to human patients and research participants, are insufficient to address the full scope of moral considerations that arise in One Health practice (Rüegg et al., 2017). One Health Ethics calls for the development of novel moral concepts and analytical tools capable of accommodating non-human moral considerability, interspecies equity, and ecological integrity as legitimate ethical concerns alongside human welfare.
Planetary Health Ethics situates human and animal health within the broader context of planetary boundaries and ecological sustainability. Drawing on Earth systems science, environmental philosophy, and global justice theory, this framework argues that the long-term health of human and non-human communities depends on maintaining the ecological conditions that sustain life on Earth. From this perspective, EIDs are not merely biomedical events but symptoms of a broader ecological crisis driven by land-use change, biodiversity loss, climate change, and unsustainable food systems. The ethical imperative extends beyond managing individual disease events to transforming the socioeconomic and political structures that create conditions favorable to pathogen emergence and spread.
The ethics of care, originally developed within feminist philosophy and nursing ethics, emphasizes relationships, interdependence, vulnerability, and contextual responsiveness as the foundations of moral reasoning (Noddings, 2013). Applied to One Health, this approach challenges the individualism and abstraction of principlist frameworks and foregrounds the relational bonds between humans and the animals, ecosystems, and communities with which they are entangled. As Anthony and De Paula Vieira (2022) demonstrate in the context of animal disaster management, an ethics of care reveals obligations toward animals arising from shared vulnerability and interdependence, obligations that are obscured by frameworks treating animals as property or resources. In EID contexts, an ethics of care approach prioritizes the needs of those most affected by outbreaks and emphasizes the maintenance of caring relationships across species boundaries in surveillance, response, and recovery.
Integrative ethical frameworks drawing on non-Western and indigenous knowledge systems represent a further significant development. Many indigenous communities maintain relational ontologies that recognize the interconnectedness of human, animal, and environmental health, and have developed ethical principles for managing human-wildlife interfaces and natural resources in ecologically sustainable and socially just ways. Emerging scholarship argues for the genuine epistemic inclusion of indigenous and local knowledge in One Health ethics, not merely as a gesture of cultural sensitivity but as recognition that these knowledge systems contain ethically significant insights about relational stewardship, reciprocity, and intergenerational responsibility that are directly relevant to EID prevention and response.
The concept of epistemic justice, drawn from the work of Fricker (Fricker, 2007), offers a further analytical lens. Epistemic injustice occurs when individuals or groups are wrongfully excluded from the production and circulation of knowledge due to their social identity or position. In One Health contexts, epistemic injustice manifests when the knowledge and experiences of marginalized communities, including small-scale farmers, indigenous peoples, women, and communities in LMICs, are systematically discounted in research, surveillance, and policy processes. Frameworks centering epistemic justice call for structural reforms that actively include marginalized voices as co-producers of knowledge and co-architects of ethical guidance.
Rights-based approaches to One Health ethics seek to ground ethical obligations in enforceable standards while extending these standards to encompass the rights of animals and ecosystems. Recent legal developments, including constitutional recognition of the rights of nature in Ecuador and Colombia and judicial affirmation of animal sentience in several jurisdictions, suggest that rights-based frameworks may increasingly provide an actionable legal basis for One Health ethical obligations toward non-human beings and ecosystems (Knox, 2017).
Taken together, these emerging frameworks share a common orientation: they seek to move One Health ethics beyond anthropocentrism, beyond methodological individualism, and beyond the limitations of principlist approaches toward more relational, pluralistic, and justice-oriented moral reasoning. However, most remain at early stages of theoretical development, and significant interdisciplinary work is required to translate them into practical guidance for One Health practitioners, policymakers, and researchers (Fig. 2).
9. Discussion
This descriptive review has mapped the ethical landscape of One Health approaches to EIDs across six interrelated domains, revealing a complex terrain of moral challenges that span disciplinary, jurisdictional, and species boundaries. The overarching finding is that while the One Health framework holds considerable promise as a basis for integrated, equitable, and sustainable responses to EIDs, its ethical dimensions remain insufficiently elaborated, inconsistently applied, and inadequately institutionalized across all domains reviewed.
A first major cross-cutting tension is the dominance of anthropocentrism, a pattern evident across all six reviewed domains. This manifests in the prioritization of human surveillance data over environmental monitoring, the default to culling as a primary zoonotic disease control strategy, and the marginalization of animal welfare in outbreak planning. Critically, as elaborated in Section 5, the ethical critique of anthropocentrism must be calibrated to context: emergency triage decisions that prioritize human lives may be defensible under the principle of rescue, while structural anthropocentrism in non-emergency governance is not. This nuanced position allows One Health ethics to acknowledge the moral complexity of emergency prioritization without conceding the broader argument for integrative governance.
A second recurring tension exists between collective welfare and individual rights, whether of human patients, research participants, or affected communities. Public health responses to EIDs routinely restrict individual autonomy in the name of collective protection, but the ethical justification for such restrictions is context-dependent and the burdens fall disproportionately on marginalized populations. Research in outbreak settings raises analogous tensions, where constrained autonomy and limited capacity for meaningful refusal challenge the adequacy of standard informed consent frameworks. Across these contexts, ethical analysis must move beyond simple trade-off models toward frameworks that actively address structural inequities and power differentials.
Third, justice in its distributive, procedural, and epistemic dimensions emerges as a central but persistently underserved ethical concern. Distributive justice concerns the fair allocation of burdens and benefits of One Health responses across human and non-human populations. Procedural justice concerns the meaningful inclusion of marginalized communities, indigenous knowledge systems, and non-human interests in decision-making. Epistemic justice concerns the recognition and inclusion of diverse knowledge traditions in the production of One Health knowledge and policy. Addressing these interrelated dimensions requires systemic change in governance architecture, research ethics, and institutional culture.
Fourth, the AMR crisis represents a cross-cutting ethical dimension that reinforces all three justice concerns. The disproportionate burden of AMR on LMICs (distributive injustice), the exclusion of LMIC health ministries from global AMR governance negotiations (procedural injustice), and the marginalization of indigenous and traditional medicine knowledge in AMR response frameworks (epistemic injustice) collectively illustrate why a robust One Health ethics must integrate AMR as a first-order ethical concern rather than a technical afterthought.
Fifth, the review consistently identifies a gap between the articulation of ethical principles and their practical implementation. Environmental ethics within One Health is described as powerfully endorsed in declaratory statements but poorly implemented in operational decisions. Research ethics frameworks are frequently compromised by institutional pressures for speed in emergency contexts. Governance structures lack the ethical infrastructure needed to navigate complex value trade-offs in a transparent and accountable manner. This implementation gap suggests that the primary ethical challenge is not the absence of relevant principles but the development of institutional mechanisms, including ethical review processes, governance frameworks, professional training, and accountability structures, capable of translating principles into consistent practice across diverse operational settings.
9.1 Ethical Perspectives from Low- and Middle-Income Countries
A limitation of the current One Health ethics literature is its reliance on frameworks developed primarily in high-income countries, which may not fully reflect the realities of LMICs. Outbreaks such as Ebola in West Africa and Nipah virus in Bangladesh demonstrate how ethical challenges are shaped by local cultural practices, community trust, livelihoods, and health system constraints (Yopa et al., 2023). Similarly, inequitable access to vaccines and therapeutics during the COVID-19 pandemic highlighted persistent concerns regarding global justice and solidarity. Furthermore, indigenous and local knowledge systems often emphasize relational understandings of human, animal, and environmental wellbeing that align closely with One Health principles (Venkatapuram, 2022). Greater inclusion of LMIC scholarship, local experiences, and indigenous perspectives is therefore essential for developing more equitable and globally relevant One Health ethical frameworks.
9.2 Limitations
Several limitations of the present review warrant acknowledgment. As a descriptive narrative review, the study does not employ the systematic search and selection protocols of a formal systematic review, and the inclusion of literature was shaped by the authors’ judgments about relevance and representativeness. The English-language focus of database searches may have resulted in the exclusion of ethically significant work published in other languages, particularly from LMIC researchers whose perspectives are central to the concerns this review identifies. The review also reflects the state of the literature as of its search dates; the field of One Health ethics is rapidly evolving, and developments occurring after the review period are not captured. Furthermore, the six-domain structure, while analytically useful, necessarily simplifies what is in practice a more fluid and overlapping ethical terrain; some ethical challenges resist categorical assignment and are addressed differently across cultural and institutional contexts. Finally, the review focuses primarily on EIDs and may not fully capture ethical considerations specific to endemic, neglected tropical diseases, or non-infectious dimensions of One Health.
9.3 Future Research Directions
Several priority areas for future research emerge from this synthesis. There is an urgent need for empirical studies examining how One Health governance bodies navigate ethical trade-offs in practice, particularly in LMIC settings where resource constraints and colonial legacies shape institutional decision-making. Methodological innovation is required to develop validated tools for integrating ethical analysis into routine One Health surveillance design, research ethics review, and policy evaluation. Interdisciplinary collaboration between ethicists, epidemiologists, veterinarians, ecologists, legal scholars, and representatives of indigenous and local communities is essential (Jesudason, 2023; Lederman, 2025). Specific priority areas include: (1) development of validated One Health ethics assessment instruments for governance contexts; (2) participatory action research with LMIC communities on ethical dimensions of zoonotic surveillance; (3) comparative analysis of AMR governance frameworks through a One Health ethics lens; and (4) longitudinal studies evaluating whether community-inclusive governance reforms produce measurable improvements in ethical outcomes.
10. Conclusion
Emerging infectious diseases at the human-animal-environment interface represent one of the most pressing ethical challenges of the contemporary period. The One Health framework offers a scientifically grounded and policy-relevant basis for integrated responses to these challenges, but its promise can only be fully realized if ethical dimensions are accorded the same rigor and institutional investment as epidemiological and operational ones. This review has demonstrated that ethical challenges in One Health approaches to EIDs are pervasive, multidimensional, and deeply interconnected, spanning animal welfare, human rights, environmental justice, governance accountability, research integrity, and the development of moral frameworks adequate to the complexity of multi-species health governance.
Several priority areas for future action emerge from this synthesis. First, there is an urgent need to develop and institutionalize ethical frameworks that genuinely integrate animal, human, and environmental health considerations, specifically frameworks that move beyond anthropocentrism without losing sight of the particular vulnerabilities and moral claims of human communities, especially the most marginalized. Second, One Health governance structures must be reformed to ensure transparency, inclusivity, and accountability, incorporating diverse knowledge systems and actively addressing global health inequities.
Third, AMR must be elevated as a core One Health ethics priority, requiring intersectoral governance that addresses the political economy of antimicrobial use in agriculture, medicine, and the environment. Fourth, research ethics frameworks require adaptation to the specific demands of One Health outbreak contexts, including expedited review mechanisms, adaptive consent procedures, meaningful community engagement, and enforceable benefit-sharing arrangements.
Finally, One Health ethics must be recognized and resourced as a distinct scholarly and policy discipline. The ethical questions surveyed in this review are not peripheral to One Health science; they are constitutive of it. How societies govern the human-animal-environment interface in the face of emerging infectious disease threats is, at its core, a moral question shaped by contested values, structural power relations, and competing visions of justice and flourishing. Meeting this challenge requires not only better science but more rigorous, inclusive, and practically grounded ethical reasoning, committed to the wellbeing of all life on a shared and profoundly interconnected planet.
Conflict of Interest
None
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Acknowledgments
None.
References
Aarons, D. (2019). Addressing the challenge for expedient ethical review of research in disasters and disease outbreaks. Bioethics, 33(3), 343–346.
Anthony, R., & De Paula Vieira, A. (2022). One health animal disaster management: An ethics of care approach. Journal of applied animal welfare science, 25(2), 180–194.
Asundi, A., & Bhadelia, N. (2020). Making emergency use of experimental vaccines safer. AMA Journal of Ethics, 22(1), 43–49.
Bambra, C., Riordan, R., Ford, J., & Matthews, F. (2020). The COVID-19 pandemic and health inequalities. J Epidemiol Community Health, 74(11), 964–968.
Basheer, A., Tran, M., Khan, B., Jentner, W., Wendelboe, A., Vogel, J., Kuhn, K., Wimberly, M. C., & Ebert, D. (2025). Comprehensive review of One Health systems for emerging infectious disease detection and management. One Health, 101253.
Bavel, J. J. V., Baicker, K., Boggio, P. S., Capraro, V., Cichocka, A., Cikara, M., Crockett, M. J., Crum, A. J., Douglas, K. M., & Druckman, J. N. (2020). Using social and behavioural science to support COVID-19 pandemic response. Nature human behaviour, 4(5), 460–471.
Bianchi, L. M. (2022). Obtaining Informed Consent for Research Studies. In Research During Medical Residency (pp. 139–156). CRC Press.
Blaxter, T., Åsbjer, E., & Fraanje, W. (2024). Animal welfare and ethics in food and agriculture. Food Ethics, 1–44.
Brill, S. A., Guerrero-Martin, S. M., & Metcalf Pate, K. A. (2019). The symbiotic relationship between scientific quality and animal research ethics. ILAR journal, 60(3), 334–340.
Criscuolo, F., & Sueur, C. (2020). An evolutionary point of view of animal ethics. Frontiers in psychology, 11, 403.
Damon, I. (2018). Preventative Medicine: Research and Use of Medical Countermeasures During an Outbreak. In Defence Against Bioterrorism: Methods for Prevention and Control (pp. 115–121). Springer.
Dawson, A., & Jennings, B. (2012). The place of solidarity in public health ethics. Public Health Reviews, 34(1), 4.
De Briyne, N., Vidović, J., Morton, D. B., & Magalhães-Sant’Ana, M. (2020). Evolution of the teaching of animal welfare science, ethics and law in European veterinary schools (2012–2019). Animals, 10(7), 1238.
Degeling, C., Johnson, J., Kerridge, I., Wilson, A., Ward, M., Stewart, C., & Gilbert, G. (2015). Implementing a One Health approach to emerging infectious disease: reflections on the socio-political, ethical and legal dimensions. BMC Public Health, 15(1), 1307.
Díaz, L., Zambrano, E., Flores, M. E., Contreras, M., Crispín, J. C., Alemán, G., Bravo, C., Armenta, A., Valdés, V. J., & Tovar, A. (2021). Ethical considerations in animal research: the principle of 3R's. Revista de investigacion clinica, 73(4), 199–209.
Diller, E. R., & Williamson, L. (2023). Supporting one health for pandemic prevention: the need for ethical innovation. Journal of Bioethical Inquiry, 20(3), 345–352.
Edwards, K. M., & Kochhar, S. (2020). Ethics of conducting clinical research in an outbreak setting. Annual Review of Virology, 7, 475–494.
Estebanez, J., & Boireau, P. (2022). One Health: A social science discussion of a global agenda. Parasite, 29, 17.
Fischhoff, B. (2012). Communicating uncertainty fulfilling the duty to inform. Issues in Science and Technology, 28(4), 63–70.
Folayan, M. O., Allman, D., Haire, B., Yakubu, A., Afolabi, M. O., & Cooper, J. (2019). Considerations for community engagement when conducting clinical trials during infectious disease emergencies in West Africa. Developing world bioethics, 19(2), 96–105.
Fricker, M. (2007). Epistemic injustice: Power and the ethics of knowing. Oxford university press.
Grace, D., Mutua, F. K., Ochungo, P., Kruska, R. L., Jones, K., Brierley, L., Lapar, M. L., Said, M. Y., Herrero, M., & Phuc, P. (2012). Mapping of poverty and likely zoonoses hotspots.
Han, Z., Wang, J., Zhang, K., & Tang, Q. (2020). The ethics of COVID-19 clinical trials: new considerations in a controversial area. Integrative Medicine Research, 9(3), 100425.
Haskins, M. H. (2020). Ethical challenges in health research during global health emergencies. South African General Practitioner, 1(3), 123–125.
Hawryluck, L., Gold, W. L., Robinson, S., Pogorski, S., Galea, S., & Styra, R. (2004). SARS control and psychological effects of quarantine, Toronto, Canada. Emerging infectious diseases, 10(7), 1206.
Jesudason, T. (2023). A one health priority research agenda for AMR. The Lancet Microbe, 4(10), e769.
Jones, K. E., Patel, N. G., Levy, M. A., Storeygard, A., Balk, D., Gittleman, J. L., & Daszak, P. (2008). Global trends in emerging infectious diseases. Nature, 451(7181), 990–993.
Kallas, E. G., & O’Connor, D. H. (2016). Real-time sharing of Zika virus data in an interconnected world. JAMA pediatrics, 170(7), 633–634.
Knox, J. H. (2017). Report of the special rapporteur on the issue of human rights obligations relating to the enjoyment of a safe, clean, healthy and sustainable environment: biodiversity report. United Nations Human Rights Council, A/HRC/34/49, Wake Forest Univ. Legal Studies Paper.
Lainé, N. (2023). The challenges of One Health. Accessing and networking with different forms of knowledge and epistemologies. CABI One Health(2023), ohcs202300016.
Lane, H. C., Marston, H. D., & Fauci, A. S. (2016). Conducting clinical trials in outbreak settings: Points to consider. Clinical trials, 13(1), 92–95.
Lederman, Z. (2025). Towards an ethical analysis of research in one health (EAROH). Journal of Bioethical Inquiry, 22(2), 395–404.
Lee, K., & Brumme, Z. L. (2013). Operationalizing the One Health approach: the global governance challenges. Health policy and planning, 28(7), 778–785.
Littler, J. (2017). Against meritocracy: Culture, power and myths of mobility. Routledge.
Machalaba, C. C., Salerno, R. H., Barton Behravesh, C., Benigno, S., Berthe, F. C., Chungong, S., Duale, S., Echalar, R., Karesh, W. B., & Ormel, H. J. (2018). Institutionalizing One Health: from assessment to action. Health security, 16(1_suppl), S–37–S–43.
Mertz, M., Hetzel, T., Alex, K., Braun, K., Camenzind, S., Dodaro, R., Jörgensen, S., Linder, E., Capas-Peneda, S., & Reihs, E. I. (2024). Interdisciplinary Animal Research Ethics—Challenges, Opportunities, and Perspectives. Animals, 14(19), 2896.
Mormina, M., Suwalowska, H., & Schneiders, M. L. (2024). Participant recruitment, consent and post-trial access to interventions. In Research ethics in epidemics and pandemics: A casebook (pp. 173–192). Springer.
Morse, S. S., Mazet, J. A., Woolhouse, M., Parrish, C. R., Carroll, D., Karesh, W. B., Zambrana-Torrelio, C., Lipkin, W. I., & Daszak, P. (2012). Prediction and prevention of the next pandemic zoonosis. The Lancet, 380(9857), 1956–1965.
Msemakweli, J. G., Mzuka, K., & Osward, A. (2024). One health approach to antimicrobial resistance: integrating human, animal, and environmental perspectives. Journal of Public Health and Community Medicine, 1(4), 132–142.
Nichol, A. A., & Antierens, A. (2021). Ethics of emerging infectious disease outbreak responses: Using Ebola virus disease as a case study of limited resource allocation. PLoS One, 16(2), e0246320.
Noddings, N. (2013). Caring: A relational approach to ethics and moral education. Univ of California Press.
Nouvet, E., Hunt, M., & Schwartz, L. (2022). “Is There Anything Else You Would Like to Add?”: The Ethics of (Not) Addressing Research Participants' Top Concerns in Public Health Emergency Health Research. Frontiers in Public Health, 10, 796414.
Organization, W. H. WHO.(2015). Global action plan on antimicrobial resistance. Geneva: World Health Organization. In: WHO Press, Geneva, Switzerland.
Organization, W. H. (2022). Joint external evaluation tool: international health regulations (2005). World Health Organization.
Organization, W. H., Programme, U. U. N. E., & Health, W. O. f. A. (2022). One health joint plan of action (2022‒2026): working together for the health of humans, animals, plants and the environment. World Health Organization.
Patz, J. A., Daszak, P., Tabor, G. M., Aguirre, A. A., Pearl, M., Epstein, J., Wolfe, N. D., Kilpatrick, A. M., Foufopoulos, J., & Molyneux, D. (2004). Unhealthy landscapes: policy recommendations on land use change and infectious disease emergence. Environmental health perspectives, 112(10), 1092.
Prainsack, B., & Buyx, A. (2012). Solidarity in contemporary bioethics–towards a new approach. Bioethics, 26(7), 343–350.
Ravinetto, R., Adhiambo, J., & Kimani, J. (2024). Research ethics preparedness during outbreaks and public health emergencies: focus on community engagement. Research Ethics, 20(4), 731–743.
Rodriguez, J. (2024). One Health ethics and the ethics of zoonoses: A silent call for global action. Veterinary Sciences, 11(9), 394.
Rüegg, S. R., McMahon, B. J., Häsler, B., Esposito, R., Nielsen, L. R., Ifejika Speranza, C., Ehlinger, T., Peyre, M., Aragrande, M., & Zinsstag, J. (2017). A blueprint to evaluate One Health. Frontiers in Public Health, 5, 20.
Saxena, A., Horby, P., Amuasi, J., Aagaard, N., Köhler, J., Gooshki, E. S., Denis, E., Reis, A. A., & Ravinetto, R. (2019). Ethics preparedness: facilitating ethics review during outbreaks-recommendations from an expert panel. BMC medical ethics, 20(1), 29.
Selgelid, M. J. (2009). A moderate pluralist approach to public health policy and ethics. Public Health Ethics, 2(2), 195–205.
Sheather, J. (2023). One Health and climate change—we need to get the ethics right. In (Vol. 383): British Medical Journal Publishing Group.
ten Have, H., & Patrão Neves, M. d. C. (2021). Animal Welfare (See Animal Ethics; Animal Research; Animal Rights). In Dictionary of Global Bioethics (pp. 121–122). Springer.
Van Boeckel, T. P., Gandra, S., Ashok, A., Caudron, Q., Grenfell, B. T., Levin, S. A., & Laxminarayan, R. (2014). Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. The Lancet infectious diseases, 14(8), 742–750.
Van Herten, J. (2021). Considerations for an ethic of One Health: towards a socially responsible zoonotic disease control Wageningen University and Research].
van Herten, J., Buikstra, S., Bovenkerk, B., & Stassen, E. (2020). Ethical decision-making in zoonotic Disease Control: how do one health strategies function in the Netherlands? Journal of Agricultural & Environmental Ethics, 33(2).
Venkatapuram, S. (2022). Ethics and global health emergencies. Current History, 121(838), 291–297.
Whitmee, S., Haines, A., Beyrer, C., Boltz, F., Capon, A. G., de Souza Dias, B. F., Ezeh, A., Frumkin, H., Gong, P., & Head, P. (2015). Safeguarding human health in the Anthropocene epoch: report of The Rockefeller Foundation–Lancet Commission on planetary health. The Lancet, 386(10007), 1973–2028.
Wolf, P. J., & Schaffner, J. E. (2019). The road to TNR: Examining trap-neuter-return through the lens of our evolving ethics. Frontiers in Veterinary Science, 5, 341.
Yeates, J. W. (2024). Animal behaviour and welfare research: A One Health perspective. Research Ethics, 20(3), 411–432.
Yopa, D. S., Massom, D. M., Kiki, G. M., Sophie, R. W., Fasine, S., Thiam, O., Zinaba, L., & Ngangue, P. (2023). Barriers and enablers to the implementation of one health strategies in developing countries: a systematic review. Frontiers in Public Health, 11, 1252428.
Zhou, Y., Frutos, R., Bennis, I., & Wakimoto, M. D. (2024). One Health governance: Theory, practice and ethics. Science in One Health, 3, 100089.